ESSR 2015 / P-0120

The “whys and wheres” of metal work around the shoulder
Congress:
ESSR 2015
Poster Number:
P-0120
Type:
Educational Poster
Keywords:
Arthritides, Complications, SPECT-CT, Plain radiographic studies, CT, Musculoskeletal joint, Infection
Authors:
N. Purohit1, I. Katsimilis1, R. Ray1, N. J. Menon2, V. T. Skiadas1, M. Sampson3; 1Southampton/UK, 2Leeds, We/UK, 3Southampton /UK
DOI:
10.1594/essr2015/P-0120

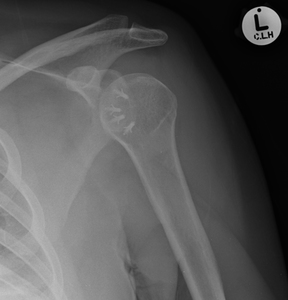
Fig. 5:
Comminuted head-splitting fracture of the left proximal humerus.

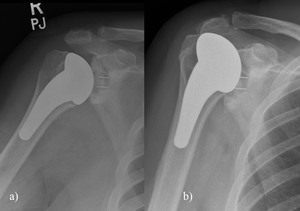
Fig. 6:
Cemented hemiarthroplasty with a standard head.

Fig. 8:
Press-fit cementless stemmed prostheses. Holes in the lateral fin of the...

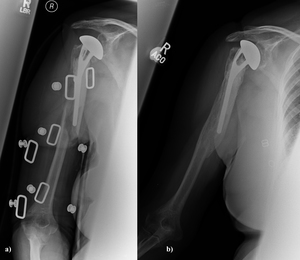
Fig. 9:
Pre and post operative images long-stem hemiarthroplasty prostheses used in a...

Fig. 10:
Long-stem prostheses for fracture or revision.
Metaphyseal window allows...
 as well as the glenoid. References: http://www.orthop.washington.edu/?q=patient-care/shoulder/shoulder-arthritis-cuff-tear-arthropathy-arthroplasty.html")
Fig. 11:
Implant in glenohumeral arthritis and rotator cuff deficiency. A special...

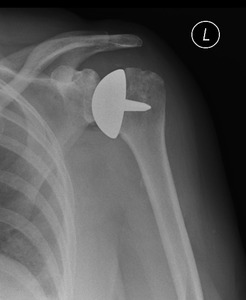
Fig. 12:
Resurfacing hemiarthroplasty of the left humeral head.

Fig. 13:
Copeland shoulder resurfacing arthroplasty.

Fig. 14:
Right glenohumeral joint arthritis. Planned for a TSA but converted to...

Fig. 15:
Right TSA for osteoarthritis. Adequate glenoid bone stock allowed for glenoid...
 with a "Fin" type system of humeral head anchorage, hydroxyapetite coated.
Bone preserving and facilitated revision.")
Fig. 16:
Tornier Simpliciti TSA for OA - intact cuff.
Stemless TSA (not humeral...
 and concave humerus (articulating cup) to reconstruct the glenohumeral joint. Preoperative images show a severely degenerative cuff tear arthropathy.")
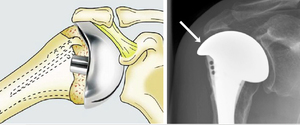
Fig. 17:
Reverse TSA. Use of a convex glenoid (hemispheric ball) and concave humerus...
 AP and Y-view radiographs of the right shoulder showing wide radiolucent lines around the glenoid peg (white arrow) b) 99mTc-HDP-SPECT/CT showing increased tracer uptake at the glenoid component-host bone interface, which was interpreted as clear sign for mechanical loosening c) AP and Y-view radiographs of the right shoulder after revision to a bipolar cup prosthesis References: http://www.internationalshoulderjournal.org")
Fig. 23:
a) AP and Y-view radiographs of the right shoulder showing wide radiolucent...
 in joint and b) dislocation of a reverse total shoulder arthroplasty")
Fig. 19:
a) in joint and b) dislocation of a reverse total shoulder arthroplasty
 Left Copeland resurfacing hemiarthroplasty. b) Painful hemiarthroplasty with evidence of glenoid sclerosis and wear. c) Postoperative radiograph following revision with a cemented glenoid component with PEG and an uncemented stemmed humeral prosthesis.")
Fig. 24:
a) Left Copeland resurfacing hemiarthroplasty. b) Painful hemiarthroplasty with...
 spiral periprosthetic fracture around the stem (Type A). Metal artifact is from a humeral brace. b) demonstrates satisfactory bony union following non-operative treatment.")
Fig. 18:
a) spiral periprosthetic fracture around the stem (Type A). Metal artifact is...
 A proximal humeral fracture treated with a proximal locking plate (PHILOS). b) c) Clear evidence of non-union on the radiograph and coronal reformatted CT.")
Fig. 21:
a) A proximal humeral fracture treated with a proximal locking plate (PHILOS)....

Fig. 30:
Metal bone anchors situated within the anteroinferior glenoid margin used for...
 following repair of the subscapularis tendon")
Fig. 29:
Multiple metallic bone anchors situated within the proximal humerus (lesser...
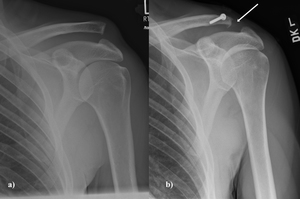
 Fracture dislocation with the fracture involving the greater tuberosity. b) The short arrow represents a cancellous screw used to fix the greater tuberosity fragment. The more distal screw with washer (long arrow) is used to augment the rotator cuff repair with a tension band suture. The suture is merely passed around the screw head.")
Fig. 26:
a) Fracture dislocation with the fracture involving the greater tuberosity. b)...
 A high grade ACJ dislocation (Grade V). b) a single cortical screw in the clavicle is used in the reconstruction of the coracoclavicular ligaments. There has been excision of the lateral end of the clavicle (white arrow)")
Fig. 25:
a) A high grade ACJ dislocation (Grade V). b) a single cortical screw in the...
 Humeral nail used in cases of pathological or b) non-pathological fractures.")
Fig. 27:
a) Humeral nail used in cases of pathological or b) non-pathological fractures.
 A displaced right proximal humeral neck fracture treated with a b) PHILOS (Proximal Humeral Internal Locking System) plate.")
Fig. 28:
a) A displaced right proximal humeral neck fracture treated with a b) PHILOS...
 Preoperative AP radiograph of a patient with anterior instability. b) Selected axial CT image shows a large bony Bankart. c,d) Post operative images following a Laterjet procedure. e) The procedure involves transfer of the coracoid with it's attached muscles to the deficient area over the front of the glenoid.
White arrow on c) demonstrates absent coracoid process.")
Fig. 31:
a) Preoperative AP radiograph of a patient with anterior instability. b)...
, humeral body (B), metal-backed glenoid component
(C) and polyethylene liner of a modular humeral component. References: Merolla G. Shoulder replacement in advanced glenohumeral osteoarthritis: current concepts review. OA Orthopaedics 2013 Jun 19;1(1):7.")
Fig. 7:
Humeral stem (A), humeral body (B), metal-backed glenoid component
(C) and...

Fig. 22:
A painful right hemiarthroplasty which had proximally migrated. Increased...

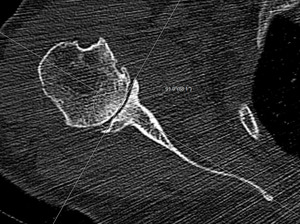
Fig. 4:
On axial 2D CT image in bone windows, just below tip of coracoid, line is drawn...
 Right TSA performed for OA. b) Proximal migration of the humeral head consistent with rotator cuff dysfunction/ tear.")
Fig. 20:
A) Right TSA performed for OA. b) Proximal migration of the humeral head...

Fig. 32:
A RTSA - area marked by the black line represents inferior scapular notching
 References: http://jbjs.org")
Fig. 33:
Radiograph of a RTSA showing posterior notching resulting from impingement of...

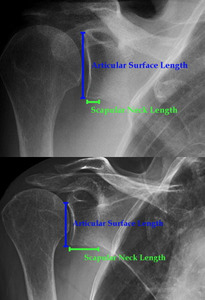
Fig. 34:
Radiograph showing short and long scapular neck length.

Fig. 35:
AP radiograph of the left shoulder after implant removal for infection,...

Fig. 36:
Preoperative AP radiograph of the left shoulder, demonstrating subsidence and...

Fig. 37:
Axillary view demonstrating anterior subluxation in a TSA with subscapularis...